 There seems to be a general movement away from targeted, pathogen-based precautions (principally screening and isolation) in the USA. This changing professional opinion was clear from the recent SHEA conference, where several leading experts gave what amounted to a collective justification for abandoning contact precautions for MRSA.
There seems to be a general movement away from targeted, pathogen-based precautions (principally screening and isolation) in the USA. This changing professional opinion was clear from the recent SHEA conference, where several leading experts gave what amounted to a collective justification for abandoning contact precautions for MRSA.
The update of the SHEA Compendium of Strategies to Prevent Healthcare-Associated Infections in Acute Care Hospitals is accompanied by a commentary from a group of leading US figures titled ‘Approaches for preventing HCAI: Go long or go wide’. In the commentary, the authors weigh the evidence and opinion for so-called ‘vertical’ (aka targeted) vs. ‘horizontal’ (aka universal) interventions (Table).
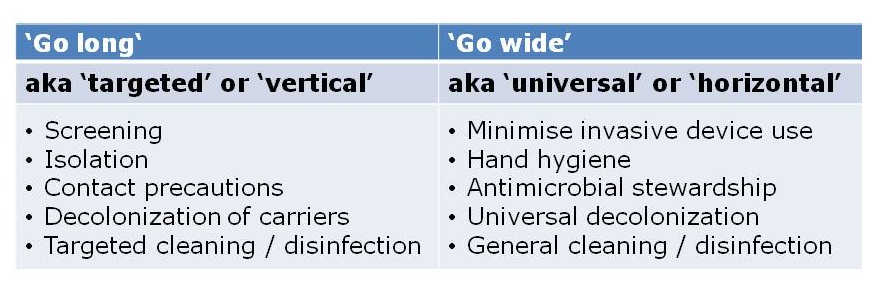 Table: Go long or go wide? Examples of targeted and universal interventions (adapted from Wenzel & Edmond, via Septimus et al.).
Table: Go long or go wide? Examples of targeted and universal interventions (adapted from Wenzel & Edmond, via Septimus et al.).
The commentary outlines the potential drawbacks of targeted approaches (such as fewer visits from healthcare workers and feelings of isolation), but doesn’t spend a lot of time discussing the potential drawbacks of universal approaches. For example, “isolation fatigue”, where a procedure loses its impact if it has to be applied to every patient. And then there’s the possibility of resistance when performing universal decolonization. This is particularly worrysome when using antibiotics, but could also be a problem when using biocides such as chlorhexidine.
I’m not ready to abandon pathogen-based targeted interventions just yet. Conceptually, it just does not make sense. If you have a patient with MRSA and a respiratory virus, chances are they will become a ‘super-spreader’. Those who favour universal approaches do make some provision for exceptional cases that really should be identified and isolated via a ‘syndromic’ approach to isolation: crudely, only isolate patients when they’re oozing. However, this syndromic approach would likely miss our ‘super-spreading’ patient, which may well result in an MRSA outbreak – that we could all do without.
Furthermore, if you have a patient who is colonized with CRE, are you brave enough to take no special precautions, as would be the case for a ‘universal only’ approach? The success of this strategy would depend on a high level of compliance with standard precautions such as hand hygiene and environmental cleaning and disinfection. Whilst sound in theory, this just doesn’t happen in the trenches; your facility is above average if your hand hygiene compliance rate is the right side of 40%. Whilst still not 100%, hand hygiene compliance is higher when patients are placed in isolation, most likely because there’s a stronger psychological trigger to comply with hand hygiene.
It’s important to note that targeted and universal approaches are by no means mutually exclusive. For example, on our ICU in London, we have been using universal chlorhexidine decolonization for a decade combined with targeted screening and isolation, and have seen a dramatic reduction in the spread of MRSA.
So, should we go long or go wide in the prevention of HCAI? The answer is both. We should optimize case for all patients, which means careful standard precations with liberal application of chlorhexidine and tight restriction of antibiotics. But we should also identify those with communicable pathogens and segregate them from others. In this regard, we have the weight of history on our side.
Image: Jeff Weese.

Hello Jon…always like reading you comments..is this disease specific isolation…a throw back to the early ’80s??..I remember that ’81-82 senior year of colleage during my MT training…what goes around comes around?? Do HCW want specific info instead of thinking for themselves? New terms to address old practices..interesting..
LikeLike
Thanks Ed, interesting comment; I wasn’t aware of a similar discussion in the early 1980s. Do you have any references to point me in the direction of some record of views at that time? I remember that some were questioning the potential for targeted interventions to prevent the spread of MRSA. For example, this article in 1998 tried to make the case that ‘Trying to control MRSA caused more problems than it solved’ http://www.ncbi.nlm.nih.gov/pubmed/9651853. At this time, I was an undergraduate student doing a dissertation on MRSA, and I thought then that this was a defeatist approach. This has been borne out by the tremendous success in bringing MRSA under control using a very targeted strategy!
LikeLike
Here’s an overview of isolation practices in US hospitals from the 1800s onwards (thanks to Ed for providing the reference): http://wonder.cdc.gov/wonder/prevguid/p0000419/p0000419.asp#head002004002000000
LikeLike
Abandoning pathogen specific control measures sounds attractive but it is questionable if it is based on science and facts. At this time we see that MRSA, VRE and ESBL are endemic in most US hospitals. CRE is the new kid on the block and in general rates are increasing rapidly despite the current control measures. The situation regarding AMR in the US is totally incomparable with the situation in my country, The Netherlands. Using pathogen specific control measures since the mergence of MRSA in the 1980’s we are still able to have total control over MRSA, VRE and CRE. For example, each year we have less than 50 cases of MRSA bacteremia in the entire country (population 17 million) and less than five of CRE. The negative effects of isolation should be taken serious but can solved by motivating doctors and nurses to give special attention to patients in isolation.
The proposed strategy in the US for me, sounds much like a surrender to antimicrobial resistance instead of a firm postion to start a real change.
LikeLike
Dear Prof Kluytmans, thank-you for taking the time to comment. I agree with you that abandoning targeted interventions feels like a surrender to antimicrobial-resistant pathogens. If universal precautions were applied perfectly all the time, then the discussion would be different. But no matter what we try, compliance with hand hygiene, environmental hygiene and other universal interventions remains sub-optimal. Therefore, I can see little option but to continue to recommend enhancing these basic procedures for specific patients to limit spread, as has been so successful in the Netherlands.
LikeLike